Wesley Smith is back again in National Review to demonstrate he does not understand genital mutilation. Last week he urged President Trump to sign HR 6100, The STOP FGM Act of 2020, which seeks to resolve the concerns of the federal court that dismissed prosecution in Michigan under the Anti-FGM Act of 1996. Within the bill:
“(a) Except as provided in subsection (b), whoever, in any circumstance described in subsection (d), knowingly—
“(1) performs, attempts to perform, or conspires to perform female genital mutilation on another person who has not attained the age of 18 years;
“(2) being the parent, guardian, or caretaker of a person who has not attained the age of 18 years facilitates or consents to the female genital mutilation of such person; or
“(3) transports a person who has not attained the age of 18 years for the purpose of the performance of female genital mutilation on such person,
shall be fined under this title, imprisoned not more than 10 years, or both.â€
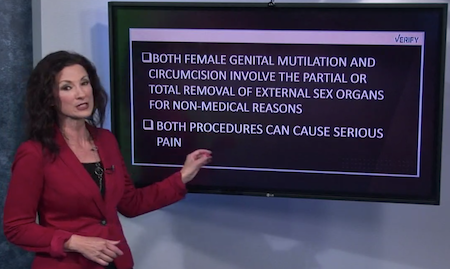
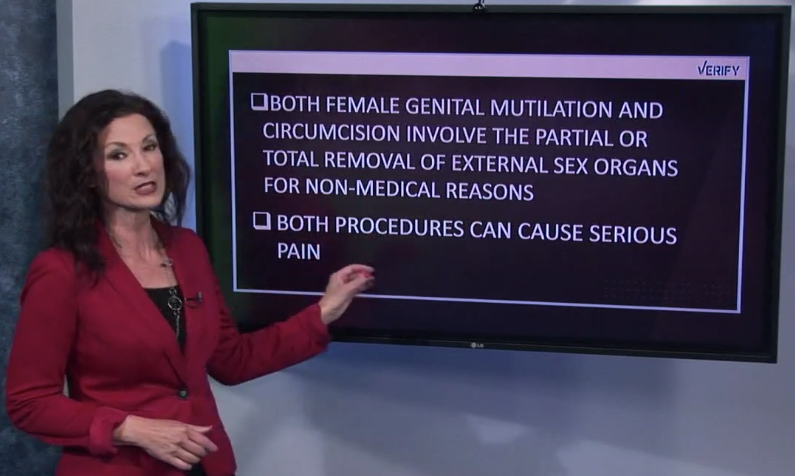
A principled individual would read that in its most direct application: non-therapeutic genital cutting on an individual who can’t consent is prohibited, full stop, without exceptions. Alas, like far too many people, Smith believes this applies to only some children, and cites this language from the bill as a foundational defense of discrimination:
It shall not be a defense to a prosecution under this section that female genital mutilation is required as a matter of religion, custom, tradition, ritual, or standard practice.
It shall not be a defense to a prosecution under this section that female genital mutilation is required as a matter of religion, custom, tradition, ritual, or standard practice to impose on a child who neither needs nor consents to surgical intervention. This is so blindingly obvious as a principle that it requires severe mental gymnastics to escape the implication to male (and intersex) children. Smith engages in those gymnastics.
I am a strong defender of religious freedom and the free exercise thereof. But the right is not absolute. The Smith case (which I oppose and hope the SCOTUS will overturn) stripped protection for religious freedom when laws are of general application — as is this bill. In other words, the bill does not single out a particular faith or group in the prohibition.
If the law protects all children, as it should, not a single word of that paragraph needs to change, excluding the parenthetical, which I’ll get to in a moment. Basically, Wesley Smith acknowledges that, under current law and precedent, restricting a religious freedom is permissible when the law is generally applicable and furthers a legitimate state interest. There is nothing more generally applicable than “you can’t mutilate the genitals of a healthy child”. And if that isn’t a compelling state interest, the state literally shouldn’t exist because it will have ceased to defend the rights of its citizens least capable of defending themselves.
Smith’s parenthetical demonstrates that he acknowledges a law prohibiting non-therapeutic genital cutting on boys without exemption for religion is the correct interpretation under current law, or he wouldn’t worry about the case in this context to protect religious “rights” at the expense of human rights he doesn’t value. In America, it’s impossible to argue that circumcision is a strictly religious practice, or that any prohibition would only stop religious parents from circumcising. Every male child can be mutilated at the request of his parents, so a law protecting his right is generally applicable. Thus, everything Smith tacks on after this is special pleading for lawless human rights violations.
That designation certainly applies to a law that prohibits the mutilation of minor girls, which, I should note, is not required by the Koran or any holy book of which I am aware and is done for the express purpose of suppressing the victim’s normal sexual functions. FGM is a direct attack on the equal intrinsic dignity of females and hence, an assault on the human exceptionalism philosophy of our societies.
He just praised the text of the bill that dismisses any claim of a religious requirement, so the fact that he’s not aware of any requirement is irrelevant. Of course, if Smith bothered to look, he’d find interpretations that conclude a requirement exists. I have no doubt Smith would – correctly – dismiss these claims as undermining this prohibition. So, his concern here is, again, special pleading to pretend that a religious requirement matters when he praised the text making it clear it doesn’t.
His belief that parents who cut their daughters always do so with the express purpose of suppressing the victim’s normal sexual functions is also unsupported with even a minimal amount of searching. That is usually the outcome, and it’s always a violation of their body and rights, but Smith assumes his opinion is fact because it’s the narrative, not because he has evidence or has studied the topic beyond a cursory review.
It’s also odd to believe that we need to defend against a direct attack on the equal intrinsic dignity of females by protecting them from what he expressly demands we continue permitting on their brothers. Where is the equality? Where is the dignity? Where is the principle he claims to defend, other than “what we do is good, what they do is bad”? If it’s wrong to cut, it’s wrong to cut.
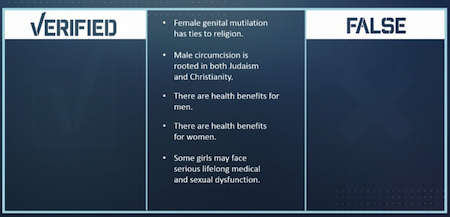
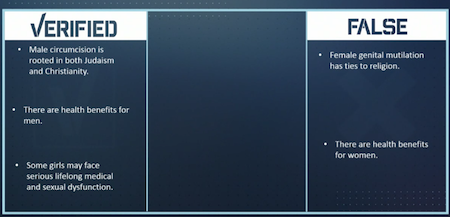
I anticipate that the “intactivists,†that is, zealots who want to outlaw male infant circumcision, will say that their cause is the same as prohibiting FGM. It is not. First, circumcision is a specific religious requirement of Judaism that brings the infant into the faith, and is also strongly promoted for religious reasons in Islam. Second, it does not destroy sexual function, nor is that the purpose of the procedure. Third, it is not undertaken as a means of oppression. Finally, medical associations believe that the decision to circumcise — regardless of religious issues — should be up to the parents as there is a modest hygienic benefit attained by the procedure.
Of course non-therapeutic genital cutting is one cause, regardless of sex. Non-therapeutic cutting of the prepuce of a non-consenting male violates his bodily autonomy the way such a surgery on a girl’s prepuce would. They both have the same property right in their own body. The only ethical position is that we won’t cut children. This shouldn’t require a law, but it does because people violate their children in this manner. And again, the state has an interest in protecting the rights of every citizen, not just those with the correct cultural favor.
And Smith already demonstrated why his concern that circumcision is a specific religious requirement is irrelevant to whether or not we should protect male minors. Laws of general applicability are generally applicable, not narrowly applicable in blatantly discriminatory ways.
Contra Smith’s opinion, circumcision destroys sexual function. Refusing to acknowledge that the normal anatomical structure of the penis, foreskin included, follows the same biological concepts as every other part of the body, including female genitalia (with foreskin), does not render the removal of the foreskin a non-destructive act inflicting no permanent harm. All surgery is battery. It is harm. The STOP FGM Act of 2020 does not make distinction for degrees of harm or intent to cause harm. The act itself is harmful to the child, and would be prohibited. Some forms of FGM are considerably more severe than a normal male circumcision. Some forms are considerably less severe. All forms will be illegal if Trump signs the bill. There is no “as long as it’s not too harmful” threshold to save male circumcision from ethical rejection.
If Smith actually cared about the complexities in this issue, he’d know that FGM is often undertaken to “improve” the girl, not to oppress her, and at the request of her female relatives over the objection of her male relatives. It still oppresses her, despite any “good” intentions, but we’re talking about the outcome, not the intent, which is what the law explicitly criminalizes.
Smith is correct that parents (generally) do not intend to oppress their sons when they circumcise. It still oppresses them. It is a form of permanent sexual control. “Your genitals will be what I approve of” is control. “You will have this potential benefit through surgical intervention, even if you’d rather just wear a condom” is control.
Having gotten this far in Smith’s shallow analysis leaves no doubt that he hasn’t assessed what “medical associations” say, such as in the APP’s policy statement. It’s an appeal to authority, except the most-often-cited authority’s policy is deeply flawed, misleading, and unethical. The very statement¹ he thinks supports a conclusion that the benefits outweigh the risks ignores the costs (i.e. harms) entirely to reach a conclusion satisfactory to people who will ponder circumcision as superficially as Smith. From the section on ethics, for example, “[r]easonable people may disagree, … how the potential medical benefits and potential medical harms of circumcision should be weighed against each other.” Reasonable people includes the human being who will live with the consequences of others choosing the most radical intervention for him as a prophylactic against mostly minor future risks that can be generally resolved with non-invasive treatments, which is the approach we take with their sisters.
So, yes. Male genital cutting is the same as female genital cutting in causing permanent harm, its ultimate violation, and the irrelevance of its religious nature on the prohibition of its imposition on children.
¹ The AAP doesn’t have a policy statement on male circumcision, because the technical report from 2012 explicitly states “[a]ll technical reports from the American Academy of Pediatrics automatically expire 5 years after publication unless reaffirmed, revised, or retired at or before that time.” It’s now eight years since this statement, and it has not been reaffirmed, revised, or retired.
{kind=link}
{kind=link}
{kind=link}