[10/19 Update: Edited for clarity and to reduce speculation since late night posting is imperfect and probably unwise.]
National Post columnist Barbara Kay used Brian Morris’ latest rehash on circumcision to repeat her ignorant thoughts on the subject. She begins by regurgitating claimed benefits, which can all be conceded here for the sake of time because they’re irrelevant to the only issue, ethics. Then:
… Dr. Morris and his American co-authors state, “We found that up to 65% of uncircumcised males might experience at least one of these [medical conditions] over their lifetime.†…
Until May 2015 Morris claimed the number as 33%. Since June 2015 he claims it’s 50% in a brochure on his website. And it’s apparently 65% in this new review. When will he settle on 100%? But more to the point, it’s obvious he likes whichever way he can claim this number because it’s flashy. “Ooooooh, 33/50/65 percent is high. Such danger!” But it’s a meaningless number in the context of non-therapeutic circumcision of boys. I assume Morris knows this. I assume Kay doesn’t, so a review of Morris’ history could help. Instead of those numbers, this is what is worth discussing here, from Morris:
Up to 10% of males reaching adulthood uncircumcised [sic] will later require circumcision for medical reasons.
Not only is the number only 10%, it’s only up to 10%. Medically necessary circumcision is rare, at any age. There is no ethical case for imposing the most radical solution without consent when at least 90% of males will never need it.
She continues:
… Their risk-benefit analysis of the procedure led them to conclude the benefits exceed the risks by about 100 to one. (In another study, published in the Journal of Sexual Medicine, Dr. Morris and colleagues found circumcision produced no adverse affect on sexual function or pleasure, a charge often leveled by anti-circumcision activist groups.)
Much like when Yair Rosenberg accepted Morris’ claim unexamined, Kay doesn’t appear to know the primary source.
But in a study Morris and Krieger rate as [highest quality], Payne et al [12], this:
… It is possible that the uncircumcised penis is more sensitive due to the presence of additional sensory receptors on the prepuce and frenulum, but this cannot be compared with the absence of such structures in the circumcised penis. …
Payne’s study published in 2007. In 2011 Kay wrote:
Set aside the rights-based rhetoric. It’s about sex: Circumcised men have greater pre-orgasmic endurance; non-circumcision permits more frequent ejaculations. …
So, circumcision either delays orgasm, assumed to be positive for all men, or has no effect on sexual pleasure. Like Morris, she appears to play “heads I win, tails you lose”.
Kay goes on to write:
… The AAP states: “The new findings show that infant circumcision should be regarded as equivalent to childhood vaccination and that as such it would be unethical not to routinely offer parents circumcision for their baby boy. Delay puts the child’s health at risk and will usually mean it will never happen.â€
That quote is not from the AAP. It’s from Prof. Morris. He wrote it in a press release more than 18 months after the AAP published its revised position statement. Kay doesn’t bother to fact check the most basic statement. [ed. note: Kay asked the online editor to correct her error.] Nor does she pursue how Morris’ quote undermines their case for non-therapeutic neonatal circumcision since he acknowledges that circumcision is rarely necessary.
Thus, while it’s inexcusable, it’s hardly shocking when she continues:
The CPS could not condemn the practice on grounds of increased morbidity. After thousands of years of what is essentially a controlled study with virtually all Jewish men, with a large percentage of Muslim men on one side, and uncircumcised men on the other, it has been unequivocally concluded that circumcision presents no health risks; quite the contrary, as we shall see.
Even Morris doesn’t pretend that circumcision “presents no health risks”. He understates them, and ignores the guaranteed harm from the removal of the foreskin (and possibly frenulum) in 100% of circumcisions. But he’s not so biased that he’ll posit such an obvious untruth. Yet, there’s Kay’s indifference masquerading as hyperbole for all to see.
… Morris’s team estimates the combined frequency of adverse events at 0.4% overall, arguing that “the cumulative frequency of medical conditions attributable to [having an intact foreskin] was approximately 100-fold higher†than the cumulative risk of circumcision.
Even if we accept the numbers, he’s arguing frequency of medical conditions attributable to the foreskin, not the frequency of medically necessary circumcision. It’s fascinating, perhaps, but a transparent obfuscation. The anti-science charge is often leveled at activists here, but soap, water, antibiotics, steroids, condoms, and so on are also science. To start with the most extreme solution at the tiny prospect of a problem sometime in the future is ridiculous.
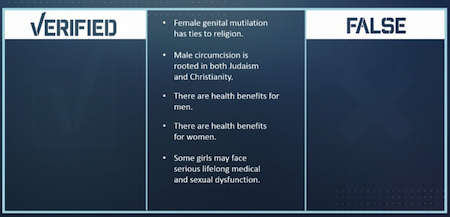
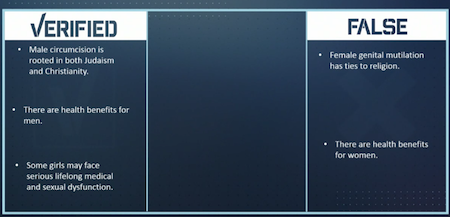
When she gets to the comparison of male and female genital cutting, she ignores the principle.
The single most irrational argument one often sees is the charge of moral equivalency between circumcision and female genital mutilation. FGM is a phenomenon that is, apart from both affecting the genitals, …
Apart from both affecting the genitals, indeed. Affecting the genitals of a healthy child who does not need or consent to the permanent alteration of said healthy genitals. Non-therapeutic genital cutting on a non-consenting individual is unethical. The individual has inherent rights to bodily integrity and autonomy from birth. Non-therapeutic circumcision violates those rights.
… quite separate from circumcision. Unlike circumcision, which removes an unnecessary piece of skin, …
Unnecessary circumcision removes a piece of skin. It’s the same words, but made objective rather than subjective. It’s the fact-based opposite of “heads I win, tails you lose”.
… in no way prevents natural and satisfying sexual function, …
In addition to calling back to the Payne study and Kay’s earlier comments about delayed orgasm, circumcision removes the foreskin, a natural part of the body. That is “natural”. Its mechanism is gone, so circumcision certainly prevents that function. And “satisfying” is subjective. Would all men prefer delayed orgasm and the loss of the foreskin? (I don’t.)
… FGM is a misogynistic practice created as a means for men to control women, …
Circumcision controls men. Its imposition is another’s assessment that the male’s body should be the way someone else prefers. It is then made that way (hopefully, except when complications occur, including possible death). The male is never asked. He is to say “thank you”, praise the imposition, and impose it on his sons as soon as they’re born.
Kay’s argument rests on control as intent rather than action. I doubt she would accept that parents cutting their daughter’s genitals for the reasons we allow them to cut their son’s genitals. She assumes their intent is always evil, but is it the intent or the act that matters here? If she believes intent with FGC is only what she writes, as she appears to believe, she should read more¹ on the topic. And then extrapolate back to the disparity in the intent and the violence of male circumcision.
… meant to prevent sexual desire and gratification in women to ensure their fidelity, and which removes a portion of the genitals absolutely vital to gratification. It is the very epitome of patriarchy, whereas circumcision is a rite of passage conceived by males for other males, and for thousands of years rooted solely in spiritually contractual language and meaning. Women who have been subjected to FGM invariably come from countries in which extreme misogyny is the norm. Circumcision carries no moral or gender-injustice baggage of this kind whatsoever.
I agree that FGM is awful. But it’s silly to repeatedly claim a definitive knowledge that male circumcision does not remove of portion of the genitals absolutely vital to gratification. She ignorantly cites bad summaries of studies and only uses groups of males circumcised at birth or as young children as reference points for this opinion. She doesn’t appear interested in males as individuals with rights and preferences of their own for their foreskins. (“Conceived by males for other males”.) Preference for the foreskin or circumcision is an individual decision. What other males prefer is only valid for themselves.
She closes by misunderstanding the ethics involved one last time, in a disgusting manner:
Parents deserve to be informed of all the evidence, pro and con, when the issue of circumcision arises. It is not necessary for the CPS to actively recommend circumcision to keep to the path of ethics and professional responsibility, but given the accumulation of evidence demonstrating the positive effects of circumcision, it would be unethical of the CPS – or any pediatricians individually – not to present the science available, or worse, to recommend against the procedure.
She’s dancing close to the silly proposition that boys have a right to grow up circumcised. The only ethical position is absolute opposition to (and prohibition of) all non-therapeutic genital cutting without the patient’s consent. It’s the right she recognizes for females. Her source (inadvertently?) recognizes that circumcision is rarely needed ever and can be (but likely won’t be) chosen later. She cites evidence of males who are dissatisfied with circumcision and being circumcised. But she ignores these in favor of her own biases. Cognitive dissonance (and a non-sequitur) is the best she can offer. She is ignorant. She should aim to be less ignorant.
¹ Consider Fuambai Sia Aahmadu, and from 2008.
{kind=link}
{kind=link}
{kind=link}