WZZM, the ABC affiliate in Grand Rapids, Michigan, has a “verify” article purporting to address the following:
The story of a female genital mutilation case in Detroit has prompted lots of questions from our viewers on what this procedure actually is and how it compares to circumcision in males. So, we set out to Verify this issue by reaching out to the experts.
WZZM “verifies” this in a surprising and predictable manner. There’s a video associated with the article. It’s what I will use as a summary for two reasons. I assume that’s what most people who arrive at the link will use. But I’ll focus on the video because it addresses what WZZM researched, not the comparison the article said they aimed to verify. (Most of the sections of the article are rote talking points. Also, I’m unconvinced the article had an editor for content because it did not have one for grammar.)
First, the on-air reporter, Val Lego, provides a summary of the two procedures.
{kind=link}
This is the surprising part. It’s accurate. As those of us who recognize the valid comparison have said, both inflict permanent harm for non-therapeutic reasons and without consent. This is where the discussion should end. If this were investigating the correct question, the comparison as posited in the article, Ms. Lego would say, “As you can see, they are comparable. They are both a violation of the child.”
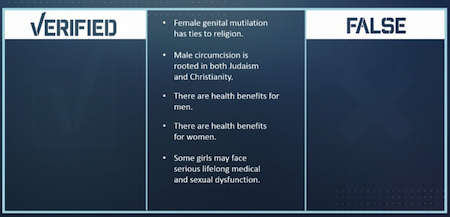
But this wasn’t investigating the correct question. Contrary to the accompanying article, WZZM sought to “verify” the difference between female genital mutilation and male circumcision. WZZM begged the question that they’re different. So, even with the ethical comparison established, the analysis works to provide the flawed, predictable psychological comfort for the viewer. Anyone with even a basic understanding of American culture can predict the outcome:
{kind=link}
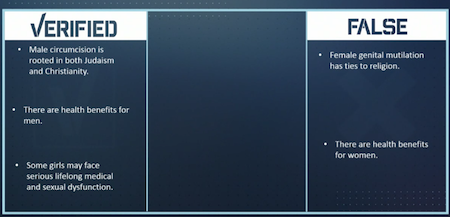
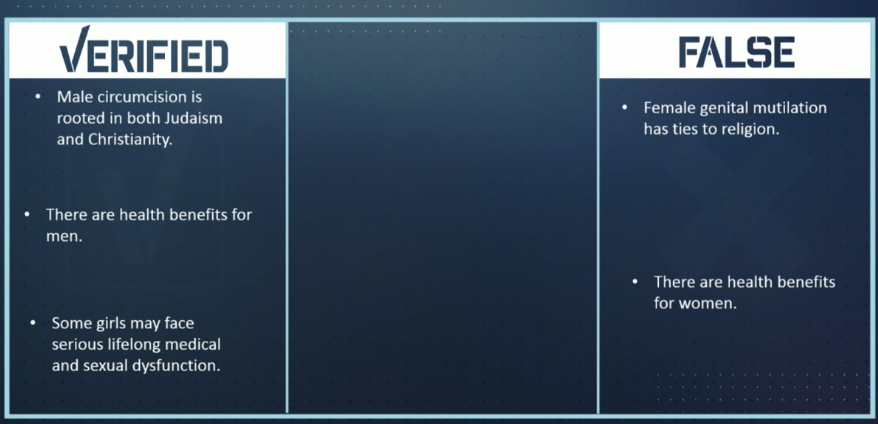
Here’s the completed list. It’s “√erified”. You got it right, didn’t you?
{kind=link}
While accurate in the merely factual sense, none of it is relevant to the question of whether child genital cutting is acceptable. The comparison established before this list demands equal protection for everyone based in the ethical principle¹, whether female or male, adult or child. Everyone has the same human rights. There are no exceptions in the right to bodily integrity for “rooted in parents’ religion”, “potential health benefits”, or “only lifelong consequences we care about”. Religious rights belong to the individual, including the choice to reject genital cutting. The potential health benefits are of subjective value² because the child is healthy. Only he may decide if he values them more than his foreskin. And permanent removal of normal body parts is harm, always. That harm occurs in varying degrees, but harm is guaranteed with every cut.
Going back to the article, it ends with this:
Dr. Megan Stubbs, sex and relationship expert, says that there is a distinct intent to curb a woman’s sexual desire when she undergoes FGM/C – women and girls may face serious, lifelong medical and sexual dysfunction.
“Men who have been circumcised typically lead happy, health lives. Circumcised men still enjoy sex, with or without a foreskin,†Dr. Stubbs states.
Again, FGM is evil in all its forms. “May face” is true here because some less-common forms of FGM do not inflict serious, lifelong harm (or inflict harm similar to circumcision). Those forms are still illegal, as they should be. Good so far.
Dr. Stubbs then counters objective harm to a female victim with “still enjoy sex” for male circumcision. It’s a ubiquitous attempt at a distinguisher, the psychological comfort to parents of boys. But Dr. Stubbs changed the criterion, going from factual statements about FGM to a subjective statement about male genital cutting. Changing form (i.e. cutting away genital parts) changes function (e.g. loss of foreskin’s gliding mechanism). Whether that’s good or not depends on the individual recipient’s opinion. Outcomes vary for every individual. Preferences for or against those outcomes differ for every individual.
The issue is proxy consent for non-therapeutic genital cutting. The first picture above makes it clear how this should be answered. It is not a separate analysis for female versus male patients. (There is perhaps a separate analysis of punishment for what is inflicted on the victim.) Without need, inflicting permanent harm on an individual via proxy consent – with unknown severity and long-term consequences – is indefensible.
No individual’s experiences (or rights) are less valid than another’s because his or her outcome isn’t typical or as severe as another’s, or because his or her parents had the perceived right intention. “Still enjoy sex” is not a Get Out of Violating Human Rights Free card. Nothing in that video or article makes me think those who oppose FGM and defend circumcision would accept FGM if potential health benefits were discovered. (It wouldn’t be ethical to research the question on children, anyway.) That’s correct because FGM/C violates the girl’s body and rights. Thinking the items in the “√erified” column excuse or differentiate male circumcision in a meaningful manner is wrong and hypocritical.
¹ Non-therapeutic genital cutting without consent of the recipient is unethical.
² Science isn’t stagnant, either. It’s realistic to imagine a future with even better ways than our existing less-invasive-than-genital-cutting options to respond to the problems prophylactic male circumcision might address.